

When Superficial Fascia Goes Deep
Superficial fascia may not get the same attention as deep fascia, but it plays an extremely important role in the organization of tissues and the structure of the body.
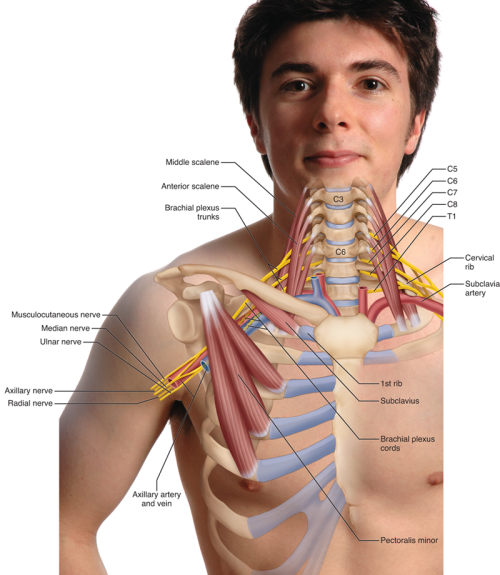
The brachial plexus of nerves and the subclavian/axillary artery and vein comprise a neurovascular bundle that is often compressed in the lower neck/upper thoracic region, causing a condition known as thoracic outlet syndrome (TOS).
There are actually four different forms of TOS, each named for the region where the compression occurs (Image 1). One is called anterior scalene syndrome because the neurovascular contents are entrapped and compressed between the anterior and middle scalene muscles. The second is called costoclavicular syndrome because the entrapment/compression occurs between the first rib (cost is Latin for "rib") and the clavicle. The third is called pectoralis minor syndrome because the entrapment/compression occurs between the pectoralis minor and the rib cage. The fourth type of TOS occurs due to the presence of a genetic anomaly that creates what is called a cervical rib, which is a formation of bone off the seventh cervical vertebra (C7).
The first three types of TOS—anterior scalene, costoclavicular, and pectoralis minor syndromes—are caused by soft-tissue postural dysfunction and will respond well to manual and movement therapy care. Therefore, the emphasis for anyone in the field of bodywork should be placed on these forms of TOS. The fourth type—cervical rib TOS—being due to a relatively rare bony anomaly (which occurs in approximately 1-2 percent of the population) is not readily treatable with manual and movement therapy and is therefore of less importance to bodyworkers.
A full awareness of the signs and symptoms of TOS cannot be understood without a somewhat in-depth knowledge of the brachial plexus; however, the major concepts can be addressed and understood. Before moving forward with this discussion, it is worth noting that symptoms, by definition, are subjective in that they must be reported by the client. For example, only the client can state if they are experiencing pain. Signs, on the other hand, are objective in that they can be measured by the therapist. For example, the strength of the client's pulse is a sign that can be felt and reported by the therapist.
Almost all peripheral spinal nerves are mixed in that they carry both sensory and motor neurons (the only exception is the C1 nerve root, which is only sensory). In this sense, they can be likened to two-lane north-south highways comprising a northbound lane that carries sensory information gathered in the periphery up to the central nervous system, and a southbound lane that carries motor information down from the central nervous system to the periphery. TOS usually involves peripheral nerve compression; therefore, the two major types of neural signs/symptoms result from sensory compression and motor compression. And, given that the brachial plexus of nerves travel to/from the upper extremity, these signs and symptoms would manifest in the upper extremity—in other words, the arm, forearm, and/or hand. Most often, upper extremity nerve compression is experienced in the hand.
Compression of a sensory neuron can cause irritation of the neuron, creating aberrant sensory impulses resulting in increased sensation, termed hyperesthesia. Examples include hypersensitivity to touch, a feeling of tingling even when no stimulus is being applied to the skin, or burning or shooting pain. When the compression is greater, it can begin to obstruct axonal flow within the sensory neuron, resulting in diminished ability of the neuron to carry impulses. This, in turn, results in diminished sensation, termed hypesthesia. This is often experienced as pins and needles, instead of a full sensation of touch, when pressure is applied to the skin. If the axonal flow is entirely blocked, numbness can result. Any altered sensation, whether it is hyperesthesia or hypesthesia, can be termed paresthesia. Because paresthesia, is by definition, something the client feels, it is a subjective symptom and must be reported by the client.
Given that motor neurons are responsible for directing muscle contraction, compression of a motor neuron would affect muscle function. If the motor neuron is irritated and creates aberrant nerve impulses, then muscle twitching (termed fasciculation) can occur. If the compression is greater, then obstruction of the axonal flow could result in the inability of the neuron to direct its muscle fibers to contract. This would result in weakness, and, perhaps in time, atrophy of the associated musculature.
Arterial blood is delivered to the upper extremity via the subclavian artery, which, as it travels distally, becomes the axillary artery, then the brachial artery, and then divides into the radial and ulnar arteries, which enter the hand. The various types of TOS can potentially compress the subclavian artery or axillary artery pathway of arterial delivery into the upper extremity. This would decrease the delivery of oxygenated arterial blood to all the tissues and cells of the upper extremity, distal to the point of compression. In light-skinned individuals, the skin's pallor might become cyanotic (bluish) and is often noticed in the hand. Decreased arterial flow can be objectively measured by feeling for the strength of the client's radial pulse at the wrist (it should be emphasized that it is the strength of the pulse, not the rate of the pulse, that is assessed). As we will see later in this article, palpating for the strength of the radial pulse is the primary means by which TOS is assessed.
Venous blood is drained from the upper extremity by veins that are similarly named to the arteries. TOS can compress the subclavian and/or axillary vein, which would result in decreased venous return and cause pooling of fluid—in other words, swelling—in the extremities. As with neural and arterial compression, this will usually be noticed in the hands.
Given that there are three different forms of soft-tissue dysfunctional TOS, there are also three different orthopedic assessment tests. I like to describe the fundamental concept of orthopedic assessment as "stress and assess." If we believe a structure is unhealthy and causing the client to experience the signs or symptoms of a condition, then the goal of our assessment test is to increase the stress on that structure to see if it reproduces or increases the client's characteristic pattern of signs and symptoms. To do this, we need to understand the underlying mechanics of the condition we are assessing. With anterior scalene syndrome, the underlying mechanism is tight anterior/middle scalene musculature; with costoclavicular syndrome, the underlying mechanism is a decreased costoclavicular space between the clavicle and first rib; and with pectoralis minor syndrome, the underlying mechanism is a tight pectoralis minor. Each of these cases results in compression on the brachial plexus of nerves (or the subclavian/axillary artery or vein).
Therefore, our orthopedic assessment tests for these conditions involve increasing the physical stress on the structures involved. For whom would we perform these TOS orthopedic assessment tests? Most often, it would be for any client who presents with upper extremity paresthesia or motor dysfunction. The most common symptom of TOS is tingling or numbness in the hand. The three orthopedic assessment tests for TOS are Adson's, Eden's, and Wright's.

Adson's test for anterior scalene syndrome places a tension stress on the scalene musculature by stretching it, thereby pulling it taut and hard against the neurovascular contents. Given that the anterior/middle scalenes are flexors of the neck in the sagittal plane, lateral flexors in the frontal plane, and contralateral rotators in the transverse plane, they would be stretched by asking the client to move the neck into extension, lateral flexion to the opposite side, and rotation to the same side (Image 3A).
It should be noted that if the client is experiencing TOS due to the presence of a cervical rib, then because the compression caused by the cervical rib occurs at the scalene musculature, Adson's test would usually show positive. Therefore, Adson's test assesses TOS due to both anterior scalene syndrome and a cervical rib. Cervical ribs can often be palpated, but definitive assessment of a cervical rib would be made by X-ray.

Eden's test for costoclavicular syndrome is performed by asking the client to assume a posture that stresses the body by decreasing the costoclavicular space. This is accomplished by asking the client to push their chest out and pull their shoulder girdles back, as if standing at attention in front of a commanding military officer (Image 3B). This pushes the first rib anteriorly against the clavicle as the clavicle is pulled posteriorly against the first rib.

Wright's test for pectoralis minor syndrome stresses the pectoralis minor by stretching it. Because the pectoralis minor is a protractor and depressor of the scapula, the client's scapula is brought back into retraction and elevation, using the client's arm as the contact (Image 3C). This tautens and hardens the pectoralis minor, as it is pulled posteriorly against the neurovascular contents. There is an alternative position for Wright's test that involves stretching and tethering the brachial plexus of nerves around the pectoralis minor by simply bringing the arm into abduction with the elbow joint flexed to approximately 90 degrees (Image 3D); this version of Wright's test is usually not as sensitive as the first version presented in Image 3C.

In each case, the therapist assesses the strength of the radial pulse. The concept is that because the brachial plexus structures lie next to the subclavian/axillary artery, then if the pulse strength is decreased due to arterial compression, we can extrapolate that the brachial plexus nerve structures must also be compressed. If the strength of the pulse decreases during the test, the test is considered positive. The test is also considered positive if the client reports the reproduction of their characteristic paresthesia pattern in the upper extremity.
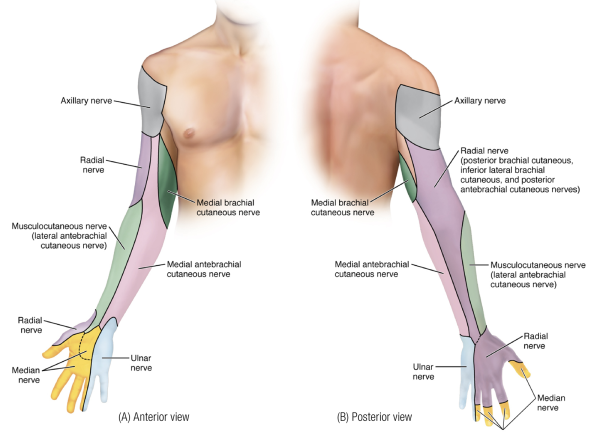
Adson's, Eden's, and Wright's tests are performed to determine which form of TOS the client is experiencing. Once the client is assessed as positive for TOS, it can then be helpful to determine which nerve is being compressed. This can be done by comparing the location of the client's paresthesia with a map of the sensory innervation of the brachial plexus nerves (Image 4). Note: this innervation pattern should not be confused with a sensory dermatomal map by spinal nerve root.
Determining the specific brachial plexus nerve that is being compressed can also be done by performing a series of orthopedic assessment tests known as brachial plexus tension tests (BPTTs). There is one BPTT for each of the brachial plexus terminal branches that enter the hand: the median, ulnar, and radial nerves. Following the concept of stress and assess, each test is performed by stressing the nerve by stretching it. Stretching a nerve is performed in a similar manner to stretching a muscle; our goal is to make it longer, and this is accomplished by knowing which side of each joint it crosses from the neck down to the fingers, and then moving these joints to increase the length of the nerve. Images 5A-C demonstrate the three BPTTs. In each case, the test would be considered positive if it recreates the client's characteristic pattern of upper extremity paresthesia. It is worth noting that these BPTTs are essentially identical to the positions used when performing nerve mobilization treatment.



Although TOS can involve neural, arterial, and/or venous compression, because nerve tissue is more sensitive to pressure, signs and symptoms of neural compression are, by far, most common. As mentioned previously, a full understanding of the signs and symptoms of TOS requires a fundamental knowledge of the brachial plexus of nerves. It is only by knowing the sensory and motor innervation patterns of the structures of the brachial plexus that a full understanding of the client's signs and symptoms can be appreciated and correlated with the TOS nerve compression that is occurring.
Unfortunately, most students and therapists are exposed to the brachial plexus as an exercise to memorize for an exam and then forget the details, without long-term understanding of its structure, its function, and its relationship to TOS. I have learned and forgotten the structure of the brachial plexus more times than I can count. After all, there are roots, trunks, divisions, cords, preterminal branches, and terminal branches. Remembering in what order these structures occur, as well as how they diverge and converge, their exact names, and what they innervate, can be a daunting task. One of the reasons so many therapists, myself included, struggle with truly learning the brachial plexus is that most all figures drawn for the brachial plexus are static and more closely resemble a metropolitan subway grid map than the brachial plexus itself.
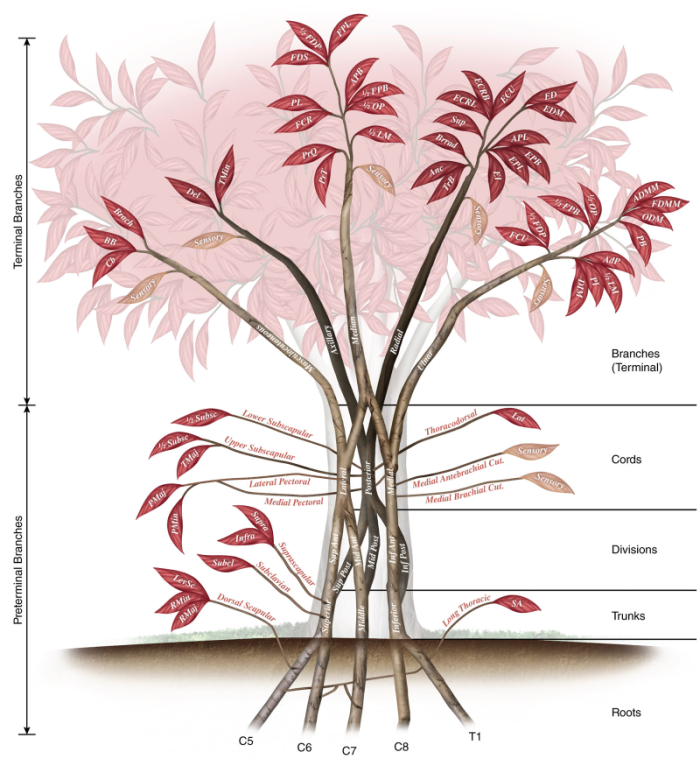
So, for the purpose of this feature, I had an illustration drawn of the brachial plexus that is anatomically correct in its labeling, but is artistically drawn as a tree (Image 2). After all, the different named parts of the brachial plexus are described as roots, trunks, divisions, cords, and branches. Having an illustration that gives expression to the named parts of the plexus and visually does so as parts of a tree can offer the therapist a powerful image, a visual touchstone that can be a major step forward toward truly learning and remembering the structural and functional intricacies of the brachial plexus.
Given how full and complicated the brachial plexus as a whole is, it is helpful to approach it a few structures at a time. For this reason, we will build up our illustration beginning literally from the ground up.
The structures of the brachial plexus, in order, are: roots, trunks, divisions, cords, and branches. More specifically, the branches at the ends of the cords are terminal branches; there are also preterminal branches that arise along the course of the brachial plexus from the roots to the cords. The structures can be seen in Image 6 and are listed in Table 1.
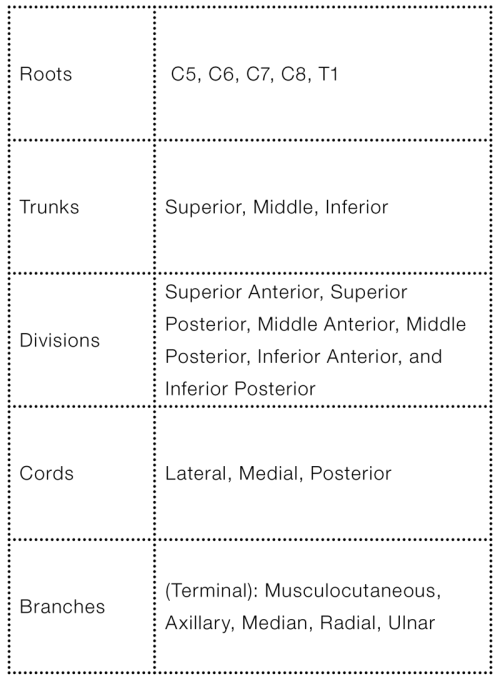
Note: only terminal branches are shown and described in Image 6 and Table 1; preterminal branches are shown in Image 2 and Table 3.
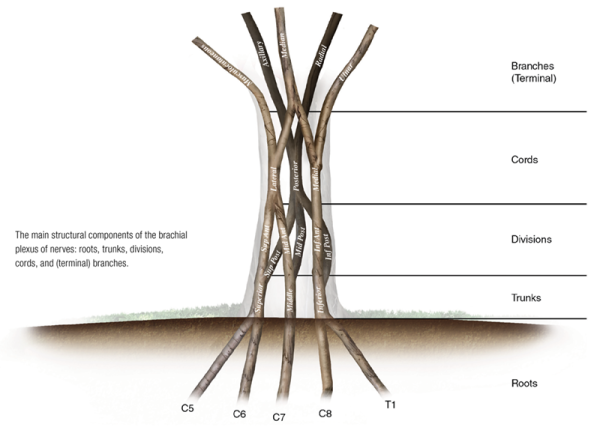
There are five nerve roots that contribute to create the brachial plexus. They are the C5, C6, C7, C8, and T1 nerve roots (Image 6).
The five nerve roots of the brachial plexus create the three trunks of the brachial plexus. They are the superior, middle, and inferior trunks.
Each of the three trunks of the brachial plexus then divides to create an anterior and posterior division. Hence, there are six divisions of the brachial plexus: superior anterior, superior posterior, middle anterior, middle posterior, inferior anterior, and inferior posterior divisions.
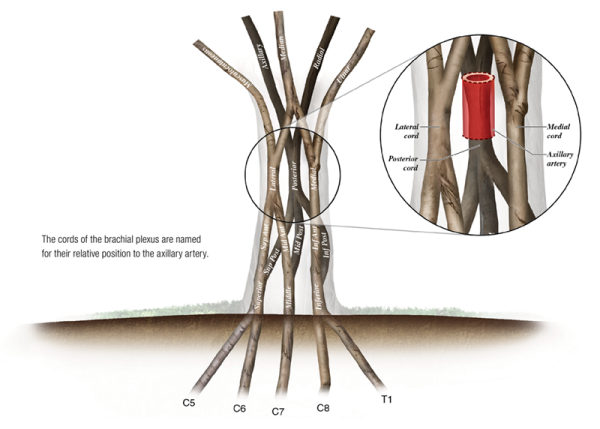
The six divisions of the brachial plexus then converge to form the three cords. They are the lateral, medial, and posterior cords. It should be pointed out that the cords are named for their relative positions to the axillary artery (Image 7).
The three cords of the brachial plexus then diverge to form the five terminal branches. They are the musculocutaneous, axillary, median, radial, and ulnar nerves.
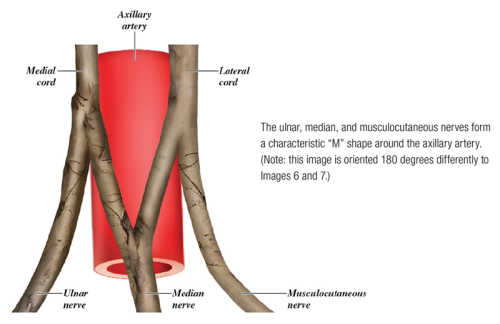
In a cadaver lab, anatomists look to identify the cords and terminal branches of the brachial plexus by locating the characteristic "M" shape of the ulnar, median, and musculocutaneous nerves around the axillary artery. The outer legs of the "M" are formed by the medial cord giving rise to the ulnar nerve and the lateral cord giving rise to the musculocutaneous nerve. The inner legs of the "M" are formed by the medial and lateral cords contributing to the median nerve (Image 8). Once these cords and branches are located and identified, the other (posterior) cord and other two terminal (radial and axillary) branches are located by looking posterior to the axillary artery. Thus, this "M" shape is the landmark for locating all three cords and all five terminal branches of the brachial plexus.
Each of the five terminal branch nerves of the brachial plexus divides to form motor neurons that innervate muscles of the upper extremity. In Image 9, each of the muscles that is innervated by a terminal branch is represented by a leaf of that branch. Note: Image 9 also shows that each of the five terminal branches also has a sensory innervation component; for more detail on these sensory innervations, please see Image 4.
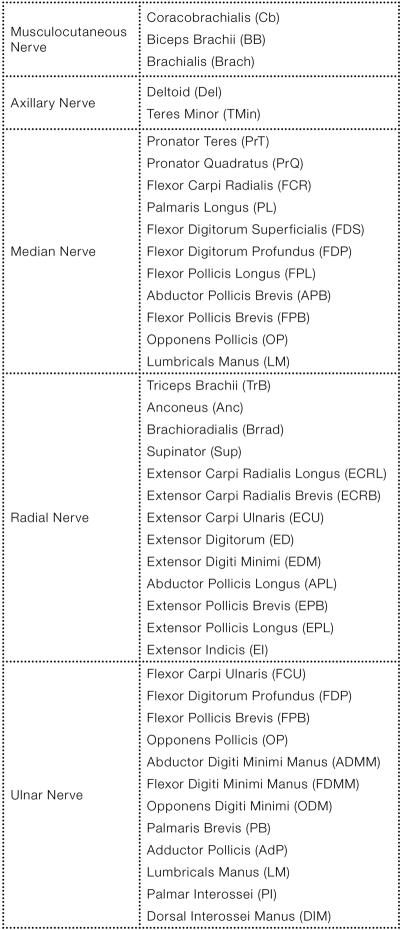
Author's note: The abbreviation listed after each name corresponds to the abbreviation used in Image 9 (as well as Image 2).
The five terminal branches of the brachial plexus are named terminal because they branch from the ends of the cords. However, there are also 11 other preterminal branches that emanate from the brachial plexus before the ends of the cords, either from roots, trunks, or along the length of the cords. These preterminal branches are shown in Image 2. Leaves indicating what muscle(s) is/are innervated by each preterminal branch (or whether it is sensory) are also indicated in this image (for more detail on these sensory innervations, please see Image 4). Thus Image 2 gives us the full expression of the structure and innervation patterns of the brachial plexus of nerves.
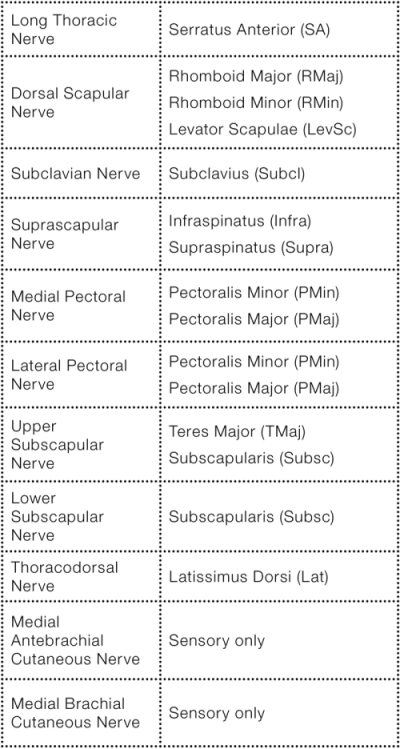
The specific muscles innervated by the terminal and preterminal branches of the brachial plexus have been described in Images 2 and 9, and listed in Tables 2 and 3. Knowing these motor innervations of the brachial plexus nerves can help us understand how TOS nerve compression can affect muscular function and assist us in finding and treating our clients' dysfunctional patterns. Most commonly, TOS will result in compression of median, radial, or ulnar nerves. Assessing the presence of TOS can then be correlated with motor dysfunction in the innervation patterns of these nerves.
The following motor innervation generalizations can be made:
The musculocutaneous nerve innervates the muscles of the anterior arm.
The median nerve innervates the muscles of the anterior forearm and the intrinsic muscles of the thenar eminence of the hand.
The ulnar nerve innervates the intrinsic muscles of the hypothenar eminence and central compartment of the hand.
And the radial nerve innervates the posterior muscles of the arm and forearm.
Author's note: slight exceptions to these rules exist (see Image 2 for the detailed muscle innervations), but they are a good starting point to learning motor innervation patterns of the upper extremity.
Although knowing anatomy for anatomy's sake is wonderful, ultimately, its importance lies in our ability to marry together the underlying science of anatomy with our hands-on manual therapy assessment and treatment techniques. By first learning anatomy (structure), physiology (function) can be figured out. By then understanding function, altered function (pathophysiology) can be figured out. Armed with an understanding of the mechanics of pathophysiology, our hands-on assessment and treatment tools can then be determined. In essence, a deeper knowledge of anatomy allows for the critical reasoning skills that then allow for creative application of our hands-on manual and movement therapy techniques.
Superficial fascia may not get the same attention as deep fascia, but it plays an extremely important role in the organization of tissues and the structure of the body.
Understanding tendons—their shapes, lengths, and organization—improves an MT’s touch vocabulary and facilitates a more skilled touch.
While the neck is a bridge, a pathway, the position of the neck and head can also indicate a multitude of other things happening beneath the surface.
Understanding fibroblasts and the extracellular matrix changes how we think about the tissue we touch.